



Imagine trying to hear your child whispering across the room, but all you catch is muffled noise. Or sitting in a quiet café and struggling to follow a conversation because low voices sound like they’re underwater. For people with otosclerosis, this isn’t imagination-it’s everyday reality. This condition, often overlooked, is one of the most common causes of hearing loss in adults under 50. And unlike typical age-related hearing decline, otosclerosis doesn’t just fade quietly-it grows silently inside your ear, locking up a tiny bone that’s supposed to move freely.
What Exactly Is Otosclerosis?
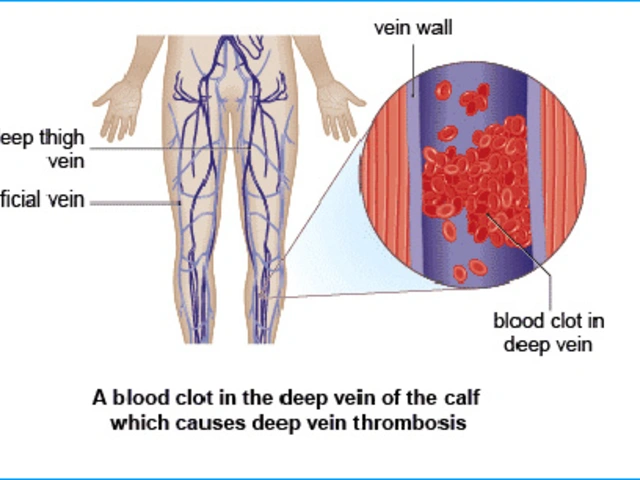
Otosclerosis is a condition where abnormal bone forms around the stapes, the smallest bone in the human body. Located in the middle ear, the stapes is only about 3.2 millimeters long-roughly the size of a grain of rice. Its job? To vibrate and pass sound from the eardrum to the inner ear. When otosclerosis kicks in, this bone starts fusing with the surrounding tissue, especially at the oval window, where it connects to the cochlea. Once it stiffens, it can’t move. And when it can’t move, sound doesn’t travel. The result? Progressive conductive hearing loss.
Unlike sudden hearing loss from an infection or trauma, otosclerosis creeps in slowly. People often don’t notice at first. They might think they just need the TV turned up. Or that their partner is mumbling. But audiograms tell a different story: a clear gap between air and bone conduction, usually between 20 and 40 decibels. That’s the signature of otosclerosis.
Who Gets Otosclerosis-and Why?
This isn’t random. Otosclerosis runs in families. About 60% of people diagnosed have a close relative with the condition. Research has pinpointed 15 genetic loci linked to it, with the RELN gene on chromosome 7 being the strongest predictor. If your mom or dad had trouble hearing in their 30s or 40s, you’re at higher risk.
It’s also far more common in women. Around 70% of cases occur in females, with peak diagnosis between ages 35 and 45. Hormones may play a role-pregnancy can accelerate the condition, which is why some women notice hearing worsening during or after childbirth.
Ethnicity matters too. People of European descent have the highest rates-up to 0.4% of the population. In contrast, African populations show rates as low as 0.1%. That’s why otosclerosis is far more frequently diagnosed in Australia, North America, and Western Europe than in other regions.
How It’s Different From Other Hearing Problems
Not all hearing loss is the same. Otosclerosis gets mistaken for other conditions all the time. Here’s how it stands apart:
- Noise-induced hearing loss: Starts with high-pitched sounds-think birds chirping or doorbells. Otosclerosis hits low tones first-voices, bass notes, whispers.
- Presbycusis (age-related): Begins after 65 and affects high frequencies. Otosclerosis shows up decades earlier and targets the opposite end of the spectrum.
- Meniere’s disease: Comes with vertigo, ringing, and fluctuating hearing. Otosclerosis? Steady, slow decline. No spinning.
- Eustachian tube dysfunction: Often misdiagnosed because both cause muffled hearing. But ETD improves with yawning or swallowing. Otosclerosis doesn’t.
A 2022 study from the American Academy of Otolaryngology found that nearly one in five patients with otosclerosis were misdiagnosed for over a year. Many went through ear drops, antibiotics, or sinus treatments before someone finally ordered an audiogram-and saw the telltale air-bone gap.

What Happens If It’s Left Untreated?
Without intervention, hearing gets worse. On average, untreated otosclerosis causes a 15 to 20 decibel decline over five years. That’s the difference between hearing a normal conversation and needing someone to shout. In 10-15% of cases, the bone growth spreads to the inner ear, damaging the cochlea. That’s when conductive loss turns into mixed or even sensorineural hearing loss-harder to fix.
Tinnitus is another common companion. A 2023 survey found 80% of otosclerosis patients deal with ringing or buzzing in their ears. For 35% of them, it’s bad enough to disrupt sleep. And while total deafness is rare, the frustration is real. One Reddit user described it as “feeling like I’m living behind a glass wall-everyone’s talking, but I can’t catch the words.”
How Is It Diagnosed?
There’s no single test. Diagnosis combines three things:
- Pure-tone audiometry: Shows a gap between how well sound travels through air versus bone. A gap of 15 dB or more is a red flag.
- Speech discrimination tests: Most patients score above 70%, meaning they understand words clearly when amplified-unlike sensorineural loss, where clarity drops even with volume.
- Temporal bone CT scan: Can reveal the early spongy bone lesions around the stapes, typically 0.5 to 2.0 mm in size.
Many primary care doctors miss it. That’s why specialists recommend seeing an otolaryngologist if you’ve had unexplained hearing loss for more than six months, especially if it’s low-pitched and getting worse.
Treatment Options: Surgery vs. Hearing Aids
Here’s the good news: otosclerosis is one of the most treatable forms of hearing loss. Two main paths exist.
Hearing Aids
For mild to moderate cases-or if surgery isn’t preferred-digital hearing aids work well. They amplify sound, especially in the low-frequency range where hearing drops. About 65% of patients start here. But they don’t stop the bone growth. They just compensate.
Surgery: Stapedotomy
The gold standard is a procedure called stapedotomy. Instead of removing the whole stapes (old method), surgeons make a tiny hole in the footplate and insert a prosthetic-often made of titanium or platinum. This lets sound pass through again.
Success rates? Up to 95% for first-time surgeries. The American Academy of Otolaryngology gives it Level A evidence-the strongest rating. Most patients regain hearing close to normal. One 45-year-old teacher in Tampa reported, “I can hear my students whispering in the back row now. I didn’t realize how much I’d been missing.”
But it’s not risk-free. About 1% of patients end up with worse hearing due to inner ear damage. That’s why surgeons spend years training-Mount Sinai requires 50 supervised stapedotomies before letting a surgeon operate alone.
There’s also a new development: the FDA-approved StapesSound™ prosthesis, coated with titanium-nitride. Early data shows a 94% success rate at 12 months-better than older models.

What About Medications?
There’s no cure, but there’s hope for slowing it down. A 2024 study in the Journal of Otology tested sodium fluoride in 120 patients. Over two years, those taking it had 37% less hearing decline than those on placebo. It’s not a treatment for everyone-side effects include stomach upset-but for younger patients with rapidly progressing cases, it’s becoming part of the conversation.
Future research is heading toward genetic screening. Experts predict that within five years, we’ll be able to identify high-risk individuals using polygenic risk scores-even before symptoms appear.
The Hidden Cost: Time, Money, and Access
Surgery costs between $8,500 and $12,000 out-of-pocket in the U.S. Insurance often covers it, but not always. In Australia, Medicare covers stapedotomy if deemed medically necessary, but wait times for specialists can stretch months.
Another challenge? Fewer surgeons are doing it. Since 2018, stapedectomy procedures have dropped 15% as younger otologists focus on cochlear implants. That means finding a skilled surgeon isn’t always easy. If you’re considering surgery, ask: “How many stapedotomies do you perform each year?”
What’s Next?
Otosclerosis isn’t going away. With improved screening and rising awareness, diagnoses are expected to grow 2.3% annually through 2030. It’s projected to remain the third most common cause of adult hearing loss through 2040.
The message is simple: if you’re under 50 and having trouble hearing low voices, don’t brush it off. Get your hearing tested. An audiogram takes 20 minutes. It could change your life.
15 Comments

Danielle Arnold
March 24, 2026 AT 02:05
So let me get this straight-we’re paying $12k to drill a hole in my skull so I can hear my cat meow again? Cool. I’ll just keep turning the TV up and blaming my husband for mumbling. At least my hearing aid doesn’t require a scalpel and a prayer.

James Moreau
March 24, 2026 AT 15:00
Really appreciate the breakdown here. I’ve been dealing with this since my late 20s and the air-bone gap was the first real clue. Took three audiologists and two years before someone said ‘otosclerosis’ out loud. It’s wild how often it’s mistaken for just ‘getting older.’

Jesse Hall
March 25, 2026 AT 05:55
This gave me chills 😭 My mom had this and didn’t get diagnosed until she was 50. Now she’s got a titanium stapes and she’s singing in choir again. If you’re under 50 and your low voices sound underwater-DON’T IGNORE IT. Get tested. Seriously.

Sean Bechtelheimer
March 25, 2026 AT 17:19
Wait… so you’re telling me this isn’t just a side effect of 5G towers and fluoride in the water? 🤔 I’ve been reading about this for weeks-turns out the government’s been hiding the real cause: microchips in hearing aids. They’re not fixing your ear-they’re listening. And that ‘titanium prosthesis’? It’s a beacon. 100% real. 🕵️♂️

Seth Eugenne
March 25, 2026 AT 17:39
Thank you for writing this with such clarity. I’ve been helping my sister navigate this diagnosis, and your breakdown of the audiogram differences? Lifesaver. The fact that speech discrimination stays high while air conduction drops? That’s the key. So many docs miss that.

Caroline Dennis
March 26, 2026 AT 12:38
Conductive vs. sensorineural. The air-bone gap is diagnostic. Stapedotomy alters impedance matching. Sodium fluoride inhibits osteoclast activity. Genetic loci: RELN, COL1A1, FSTL1. You’re not ‘just losing hearing’-you’re experiencing a biomechanical cascade. Get the CT. Don’t wait.

Kenneth Jones
March 27, 2026 AT 20:36
Everyone’s acting like this is some rare mystery. It’s not. It’s genetic. It’s in your DNA. If your mom had it, you’re next. Stop wasting time with hearing aids. Get the surgery. Or keep living in a muffled world. Your call.

Mihir Patel
March 29, 2026 AT 21:27
OMG I JUST REALIZED I HAVE THIS 😭 I thought my bf was just being quiet but nooo… I’ve been asking him to repeat everything since 2021. I’m getting an audiogram tomorrow. Thank you for this post!! I’m not crazy!! 🥲🫶

Kevin Y.
March 30, 2026 AT 02:25
Thank you for taking the time to compile such a comprehensive and clinically accurate overview. The inclusion of the 2024 sodium fluoride data, the distinction between conductive and mixed loss, and the surgical success metrics are invaluable. This is precisely the kind of resource we need to bridge the gap between patient experience and medical literacy.

Raphael Schwartz
March 30, 2026 AT 23:24
US healthcare is a joke. $12k for a fix that should be free? Meanwhile, China’s doing it for $200. Why? Because they don’t have greedy doctors. We’re being exploited. Get your hearing tested and then move to Canada.

Marissa Staples
April 1, 2026 AT 14:37
I wonder if this is just evolution catching up. Maybe our ears are slowly adapting to a quieter world-no need to hear whispers anymore. Or maybe we’re just getting better at pretending we’re listening.

Rachele Tycksen
April 2, 2026 AT 19:59
i got this too and its so weird how you just start thinkin ur partner is being rude when theyre not lol

Grace Kusta Nasralla
April 4, 2026 AT 14:37
It’s not just about hearing. It’s about being seen. When you can’t catch the words, you start to feel invisible. Like you’re not part of the conversation. Like you’re not real. That’s the worst part.

Korn Deno
April 6, 2026 AT 02:10
The real tragedy isn’t the bone growth-it’s how we treat hearing loss as a personal failure rather than a biological one. We blame the individual for not listening, not the system for not diagnosing. We’ve normalized silence instead of fixing the mechanism.

Aaron Sims
April 6, 2026 AT 13:28
Oh, so now it’s ‘genetic’? Funny how that’s the official story… but what about the 1997 CDC memo on barium exposure in dental fillings? And the 2003 patent filed by a pharmaceutical company for ‘bone-stimulating agents’-wait, that’s just ‘fluoride’? Coincidence? I think not. Also, the ‘titanium prosthesis’? It’s a micro-transmitter. You’re being tracked. And the 95% success rate? That’s just the number they want you to believe.
Write a comment